
Most people have had a knot in their neck or shoulder that just won’t go away. You rub it, stretch it, sleep on a different pillow, and it’s still there two weeks later. That knot has a name and a clinical explanation: it’s a myofascial trigger point, and trigger point therapy exists precisely because rubbing harder, or rubbing more generally, tends to miss the underlying neuromuscular problem entirely.
Trigger point therapy is the practice of locating and treating these hyperirritable spots within muscle tissue to relieve both local pain and referred pain felt in distant areas. At Complete Bodywork in Orem, Utah, trigger point release is one component of a full neurosomatic assessment that looks at the whole body’s compensation patterns rather than a quick fix applied in isolation. That distinction matters, and by the end of this article, you’ll understand why.
What a trigger point actually is
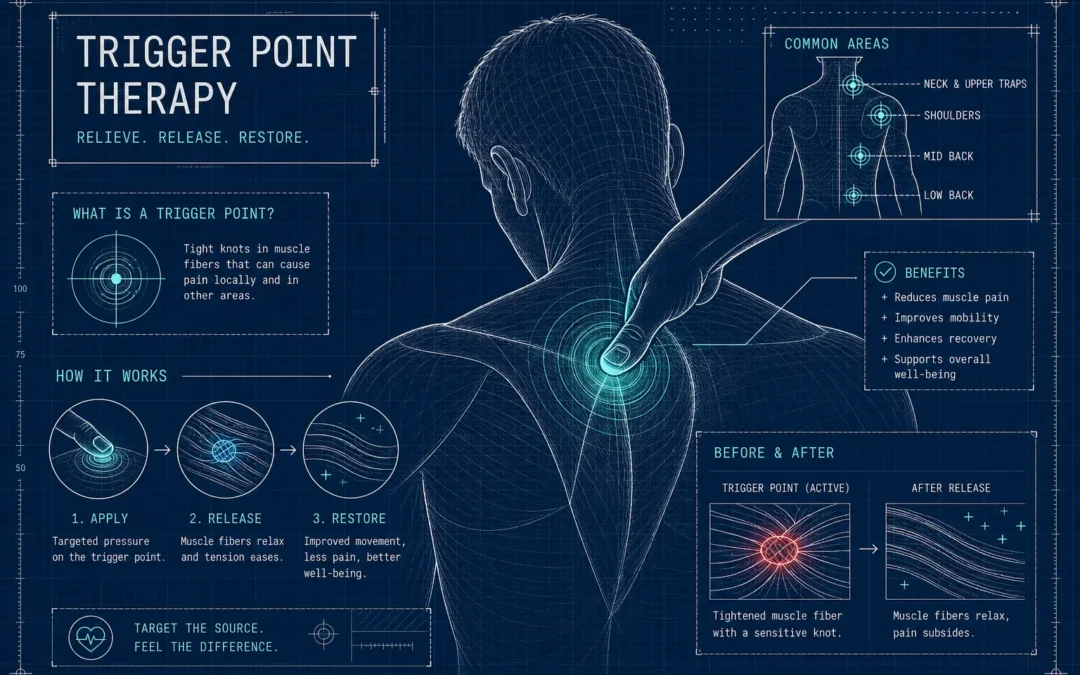
The clinical definition is a discrete, hyperirritable spot within a palpable taut band of skeletal muscle that produces localized pain and referred pain when pressed. This isn’t generalized muscle tightness or muscle knot discomfort in a vague sense. It’s specific, identifiable, and diagnosable by a trained clinician through hands-on palpation.
There are two types. Active trigger points cause pain at rest and produce referred pain patterns on pressure. A knot in your upper trapezius, for example, can send pain up into your skull and behind your eye. Latent trigger points are dormant and don’t cause spontaneous pain, but they restrict movement and create muscle weakness that often exceeds what you’d expect from something that “doesn’t hurt.” Active points need relief now; latent points need treatment to prevent them from becoming active later. Both types need attention, but for different reasons.
Clinicians identify trigger points using four physical signs: a palpable taut band, the jump sign (involuntary flinch under pressure), the local twitch response (a visible muscle contraction under snapping pressure), and a predictable referred pain map. While palpation remains the primary diagnostic method, diagnostic ultrasound and surface EMG can sometimes demonstrate focal abnormalities and may be used adjunctively. This is exactly why treating the wrong spot is so common when people self-diagnose without professional guidance.
How trigger point therapy works
A trigger point is thought to be a focal zone of sustained muscle contraction where normal blood flow has been disrupted. Metabolic waste builds up, local nerve endings become sensitized, and the muscle locks into a self-reinforcing contraction cycle that may not reliably resolve without some form of intervention.
Physiology of trigger points
Manual pressure or dry needling interrupts that contraction cycle. The sustained compression stimulates blood flow, activates the body’s endogenous pain-relief system, and elicits the local twitch response that signals the muscle fiber to reset, mechanisms described in mechanistic research on both manual therapy and dry needling. Trigger point massage techniques apply this principle through targeted, sustained pressure on one hyperirritable spot, held for 30 to 60 seconds, to produce a specific tissue response. This is physiologically different from general massage: broad Swedish techniques increase circulation and feel good, but they don’t target the specific neuromuscular dysfunction that drives myofascial pain syndrome.
Manual techniques vs. dry needling
Both manual trigger point therapy and dry needling aim to disrupt the same dysfunctional cycle. Manual pressure uses a finger, thumb, or tool applied directly to the taut band. Dry needling uses a fine filiform needle inserted into the trigger point to provoke a local twitch response. The delivery differs; the physiological target is the same. Self myofascial release methods, foam rollers, lacrosse balls, or sustained finger pressure, follow this same logic at a lower intensity, making them useful for maintenance between professional sessions.
What the evidence says about trigger point treatment
Systematic reviews from 2021 onward support dry needling for short- and medium-term pain relief in neck and shoulder trigger points. It outperforms stretching and TENS, and performs comparably to manual therapy for most pain outcomes. Manual trigger point therapy shows similar results to other conservative treatments and is generally considered a valid first-line approach for myofascial pain syndrome.
Interestingly, research suggests the mechanical effect of the needle itself, not the medication, drives much of the relief in injection-based approaches. This bridges into the honest caveat about injection evidence: trigger point injections (wet needling with lidocaine or similar anesthetics) show stronger medium-term outcomes than dry needling for stubborn cases, according to several comparative systematic reviews, though the overall quality of that evidence is low to moderate. The American Academy of Family Physicians recommends reserving injections for patients whose pain hasn’t responded to less invasive options and should not be used as a starting point.
One honest note: that low-to-moderate evidence rating applies across all three approaches. That doesn’t mean these treatments don’t work. It means confident claims about one method being definitively superior require caution. What the research consistently supports is that early trigger point treatment matters and a multimodal approach outperforms any single technique used in isolation.
Safe at-home techniques worth trying
The most clinically supported self-release method is sustained pressure. Follow these steps to do it safely.
- Locate the tender spot using gentle circular pressure around the sore area.
- Choose your tool: a finger, knuckle, lacrosse ball, or foam roller depending on the location.
- Apply moderate steady pressure at roughly 50 percent of your maximum comfort tolerance. The sensation should feel like a productive ache, not sharp or electric pain.
- Hold for 30 to 60 seconds, breathing normally, until you feel a softening or reduction in discomfort.
- Release gradually, then follow with a gentle stretch of that muscle.
Two to three repetitions per session is enough. Applying more pressure does not produce better results and risks tissue irritation. Stop immediately if the pain feels sharp or radiating rather than dull and localized. Avoid self-treating anywhere near the spine without professional guidance, and skip this entirely if you have a recent injury, active inflammation, or are post-surgical in that area.
When to stop self-treating and see a specialist
If the same trigger points keep returning, if pain refers to multiple sites, or if discomfort has persisted for more than a few weeks despite consistent self-care, the pattern likely involves more than one isolated knot. Chronic myofascial pain typically reflects underlying postural imbalances, altered length-tension relationships across connected muscle groups, and nervous system sensitization that no amount of self myofascial release fully addresses on its own.
This is where a neurosomatic assessment changes the picture. At Complete Bodywork, Benjamin begins every new client relationship with comprehensive postural measurement and a full-body neuromuscular evaluation. Trigger point therapy becomes one tool within a personalized plan built around your specific compensation patterns, not a generic protocol. Research on multimodal, individualized care consistently shows benefit for patients with chronic myofascial pain who haven’t responded to single-modality approaches, and this whole-system framework reflects that evidence.
When to seek a specialist near you
Regardless of where you live, the decision to move from self-care to professional trigger point therapy generally comes down to three signals: pain that refers consistently to a distant site, symptoms that return within days of self-treatment, or functional limitations that affect work or sleep. A qualified practitioner, whether a neurosomatic therapist, physical therapist trained in dry needling, or a licensed massage therapist specializing in trigger point massage techniques, can assess which muscles are primary drivers versus compensating for dysfunction elsewhere.
The bottom line on trigger point therapy
Trigger points are specific, clinically definable, and treatable, supported by growing expert consensus and a steadily improving body of systematic research. Self-release techniques work well for mild or occasional muscle tension, and the step-by-step method above gives you a safe place to start. But trigger point therapy applied in isolation rarely solves chronic pain. The more useful question is why those trigger points keep forming in the first place.
If you’re in the Orem, Utah area and ready to get that answer, Complete Bodywork offers a free initial consultation. Benjamin at Complete Bodywork will take your full history, assess your postural patterns, and build a plan around the root cause, not just the symptom you walked in with.

